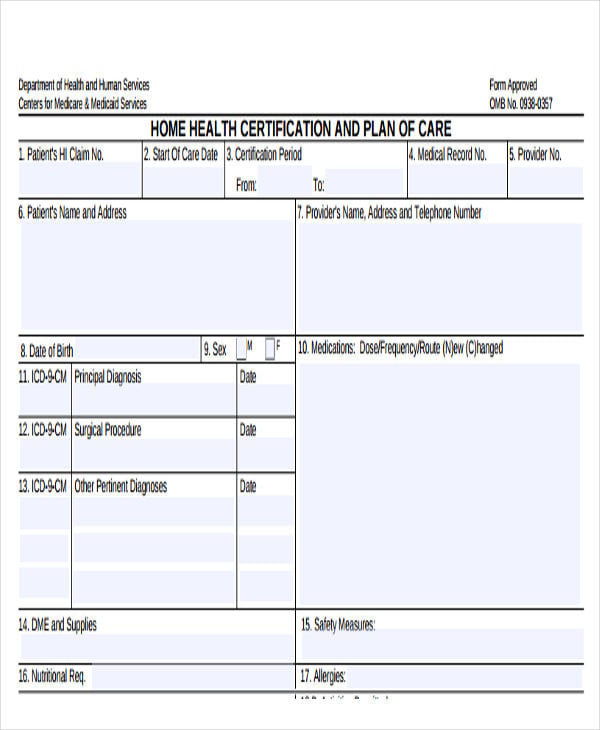
Printable Home Health Aide Care Plan Template - This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or.
I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Aide care plan patients name:
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or.

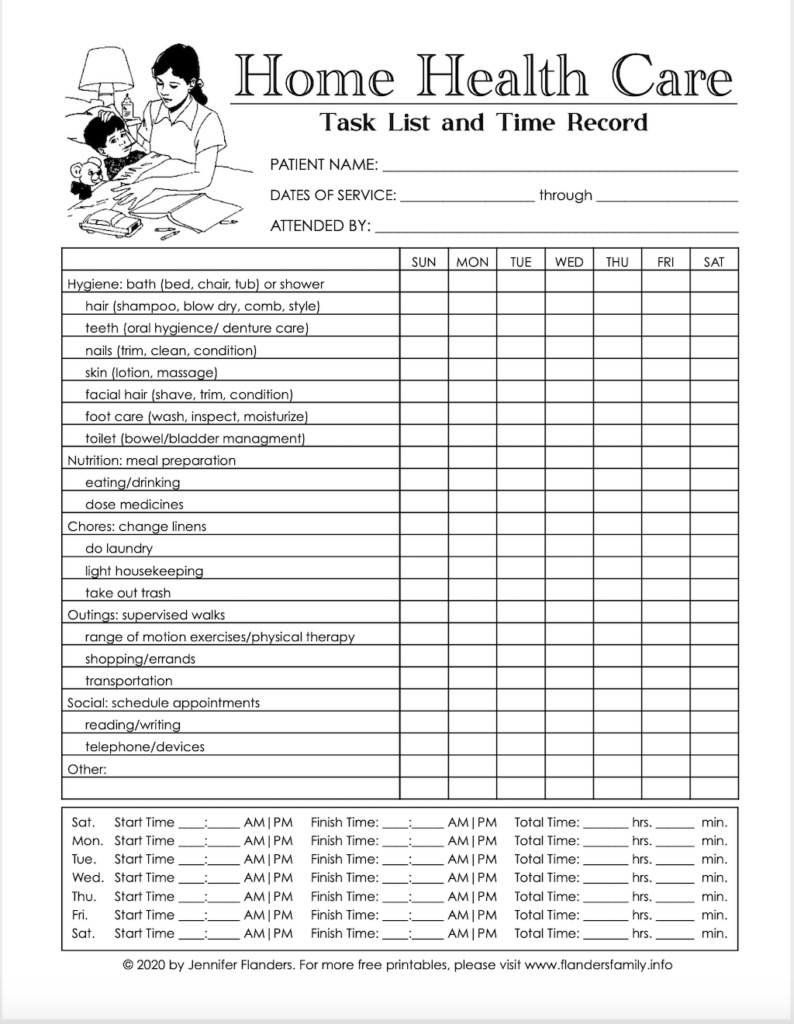
Printable Home Health Care Forms Templates
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. Aide care plan patients name:

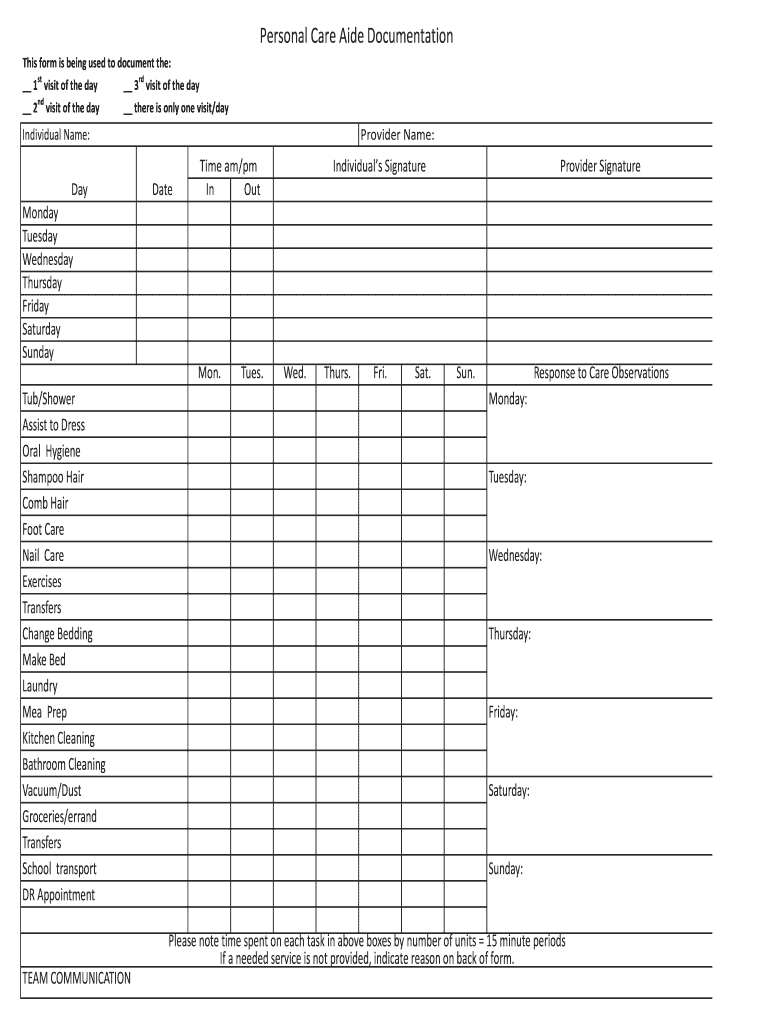
Printable Home Health Aide Care Plan Template
Aide care plan patients name: This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or.

Printable Home Health Care Forms Templates
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. Aide care plan patients name:

Printable Home Health Aide Care Plan Template
Aide care plan patients name: This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or.
Printable Home Health Aide Care Plan Template
I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Aide care plan patients name:
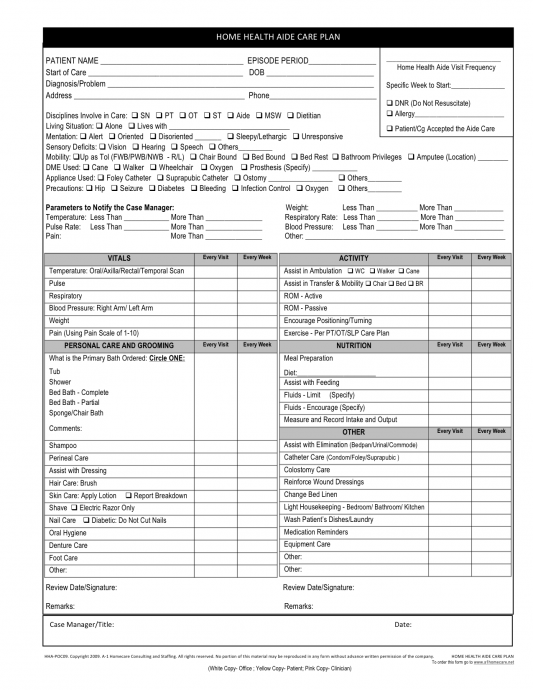
Home Health Aide Care Plan Template
Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.

Printable Home Health Aide Care Plan Template Printable Word Searches
Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.
Home Health Aide Care Plan Template
Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.
Printable Home Health Aide Care Plan Template
I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. Aide care plan patients name: This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.

Printable Home Health Aide Care Plan Template Free Printable
Aide care plan patients name: I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.
Aide Care Plan Patients Name:
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. I certify/recertify that this patient is confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech therapy or.